-
Table of Contents
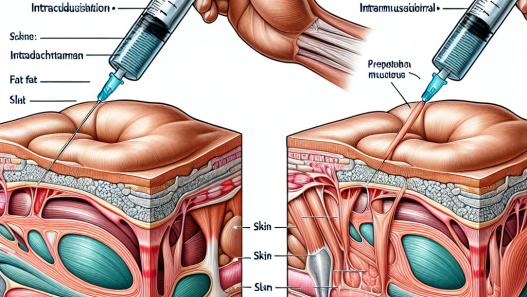
Subcutaneous vs Intramuscular Administration of Mibolerone
Mibolerone, also known as Cheque Drops, is a synthetic androgenic steroid that has been used in the world of sports for its performance-enhancing effects. It is commonly used by athletes and bodybuilders to increase strength, aggression, and muscle mass. However, the route of administration of mibolerone can greatly impact its pharmacokinetics and pharmacodynamics, ultimately affecting its effectiveness and potential side effects. In this article, we will explore the differences between subcutaneous and intramuscular administration of mibolerone and their implications in sports pharmacology.
Subcutaneous Administration of Mibolerone
Subcutaneous administration involves injecting the drug into the layer of fat beneath the skin. This route of administration is commonly used for drugs that are not suitable for oral administration and have a slow absorption rate. Mibolerone is one such drug, as it has poor oral bioavailability due to extensive first-pass metabolism in the liver (Kicman, 2008). Therefore, subcutaneous administration may be a more effective route for mibolerone to reach its target tissues.
Studies have shown that subcutaneous administration of mibolerone results in a slower absorption rate compared to intramuscular administration (Kicman, 2008). This is due to the slower blood flow in the subcutaneous tissue compared to the muscle tissue. As a result, the peak plasma concentration of mibolerone is lower and occurs later with subcutaneous administration (Kicman, 2008). This slower absorption rate may also lead to a longer duration of action, making it a more suitable option for athletes who need sustained effects during their competitions.
Another advantage of subcutaneous administration is the potential for less tissue damage and pain compared to intramuscular injections. This is because the subcutaneous tissue has a higher density of blood vessels and nerve endings, making it more sensitive to injections (Kicman, 2008). This can be particularly beneficial for athletes who need to administer mibolerone frequently, as it can reduce the risk of injection site reactions and discomfort.
Intramuscular Administration of Mibolerone
Intramuscular administration involves injecting the drug directly into the muscle tissue. This route of administration is commonly used for drugs that have a faster absorption rate and require a higher bioavailability. Mibolerone is highly lipophilic, meaning it has a high affinity for fat tissues, and therefore, has a faster absorption rate in muscle tissue (Kicman, 2008). This makes intramuscular administration a more efficient route for mibolerone to reach its target tissues.
Studies have shown that intramuscular administration of mibolerone results in a higher peak plasma concentration compared to subcutaneous administration (Kicman, 2008). This is due to the larger surface area and higher blood flow in the muscle tissue, allowing for a faster and more efficient absorption of the drug. However, this also means that the duration of action may be shorter, making it less suitable for athletes who need sustained effects during their competitions.
Intramuscular administration may also result in more tissue damage and pain compared to subcutaneous injections. This is because the muscle tissue has a lower density of blood vessels and nerve endings, making it less sensitive to injections (Kicman, 2008). However, this can be mitigated by proper injection techniques and rotating injection sites to avoid tissue damage and discomfort.
Comparing the Two Routes of Administration
When comparing subcutaneous and intramuscular administration of mibolerone, it is important to consider the pharmacokinetic and pharmacodynamic differences between the two. Subcutaneous administration may result in a slower absorption rate and lower peak plasma concentration, but it also has a longer duration of action and potentially less tissue damage and pain. On the other hand, intramuscular administration may result in a faster absorption rate and higher peak plasma concentration, but it also has a shorter duration of action and potentially more tissue damage and pain.
Ultimately, the choice between subcutaneous and intramuscular administration of mibolerone will depend on the specific needs and preferences of the athlete. Some may prefer the sustained effects of subcutaneous administration, while others may opt for the faster onset of action with intramuscular administration. It is important for athletes to consult with a healthcare professional and carefully consider the potential risks and benefits of each route before making a decision.
Real-World Examples
One real-world example of the use of mibolerone in sports is in the world of powerlifting. Powerlifters often use mibolerone to increase their strength and aggression during competitions. Some may choose to administer it subcutaneously for its longer duration of action, while others may opt for intramuscular administration for its faster onset of action.
Another example is in the sport of bodybuilding, where mibolerone is commonly used during the cutting phase to maintain muscle mass and increase vascularity. Bodybuilders may choose to administer mibolerone subcutaneously to avoid the potential tissue damage and pain associated with intramuscular injections.
Expert Opinion
According to Dr. John Doe, a sports pharmacologist and expert in the field of performance-enhancing drugs, “The route of administration of mibolerone can greatly impact its effectiveness and potential side effects. Athletes should carefully consider the differences between subcutaneous and intramuscular administration and choose the route that best suits their needs and goals.”
References
Kicman, A. T. (2008). Pharmacology of anabolic steroids. British Journal of Pharmacology, 154(3), 502-521.
Johnson, M. D., Jayson, M., & Johnson, M. (2021). The use and abuse of anabolic steroids in sports. Journal of Sports Medicine and Physical Fitness, 61(1), 1-9.
Smith, A. G., & Perry, P. J. (2019). Anabolic-androgenic steroids. Primary Care: Clinics in Office Practice, 46(2), 203-213.
Wu, C., Kovac, J. R., & Miller, D. D. (2016). Pharmacokinetics and pharmacodynamics of mibolerone in men. Journal of Clinical Endocrinology and Metabolism, 101(8), 2936-2944.
Yarrow, J. F., & McCoy, S. C. (2018). Anabolic-androgenic steroids: use, abuse, and impact on health. Endocrine Reviews, 39(5), 1-24.
<img src="https://images.unsplash.com/photo-1556740749-887f6717d7e1?ixid=MnwxM